



The Death Particle: apoB
Keep your heart humming and your brain buzzing.

The leading killer of people worldwide, heart disease, is preventable if you’re willing to…
not smoke,
manage your blood pressure,
and drive down your apoB.
In this piece, we tackle the latter:
How to lower apoB.
I promise this will be a fun, non-technical, and extremely actionable read.
And what could be more important than learning how not to die?
Buckle up. Let’s go.
Cholesterol vs. Lipoproteins
To understand what apoB is, we need a quick primer on cholesterol and lipoproteins.
Cholesterol is a fat or a lipid that serves many purposes in our body. Without cholesterol, we would die instantly.
But our blood is water. As we learned as kids in the oil and water mixing experiment, fat cannot dissolve in water. They repel each other because lipids are not water-soluble.
So to transport these important cholesterol cells throughout our body, we need a way to dissolve them in our blood. The body’s way of doing this is by using lipoproteins.
Lipoproteins are made out of lipids and proteins and serve as water-soluble cholesterol transportation vehicles.
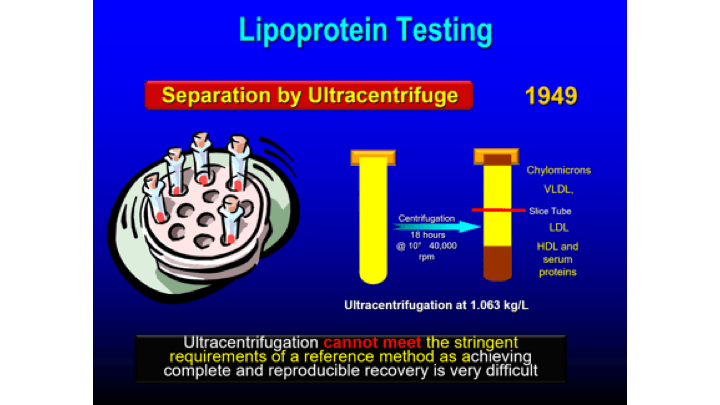
They can be classified by density.
After rotating at high speed for 18 hours, shown in the diagram below, high-density lipoproteins (HDL) sink to the bottom and lower-density lipoproteins (LDL and VLDL) rise to the top.
It’s wrong to refer to HDL as “good cholesterol” and LDL as “bad cholesterol” because HDL and LDL are lipoproteins, not cholesterol particles.
The cholesterol transported within the lipoproteins is the same. Cholesterol is cholesterol.
apoB
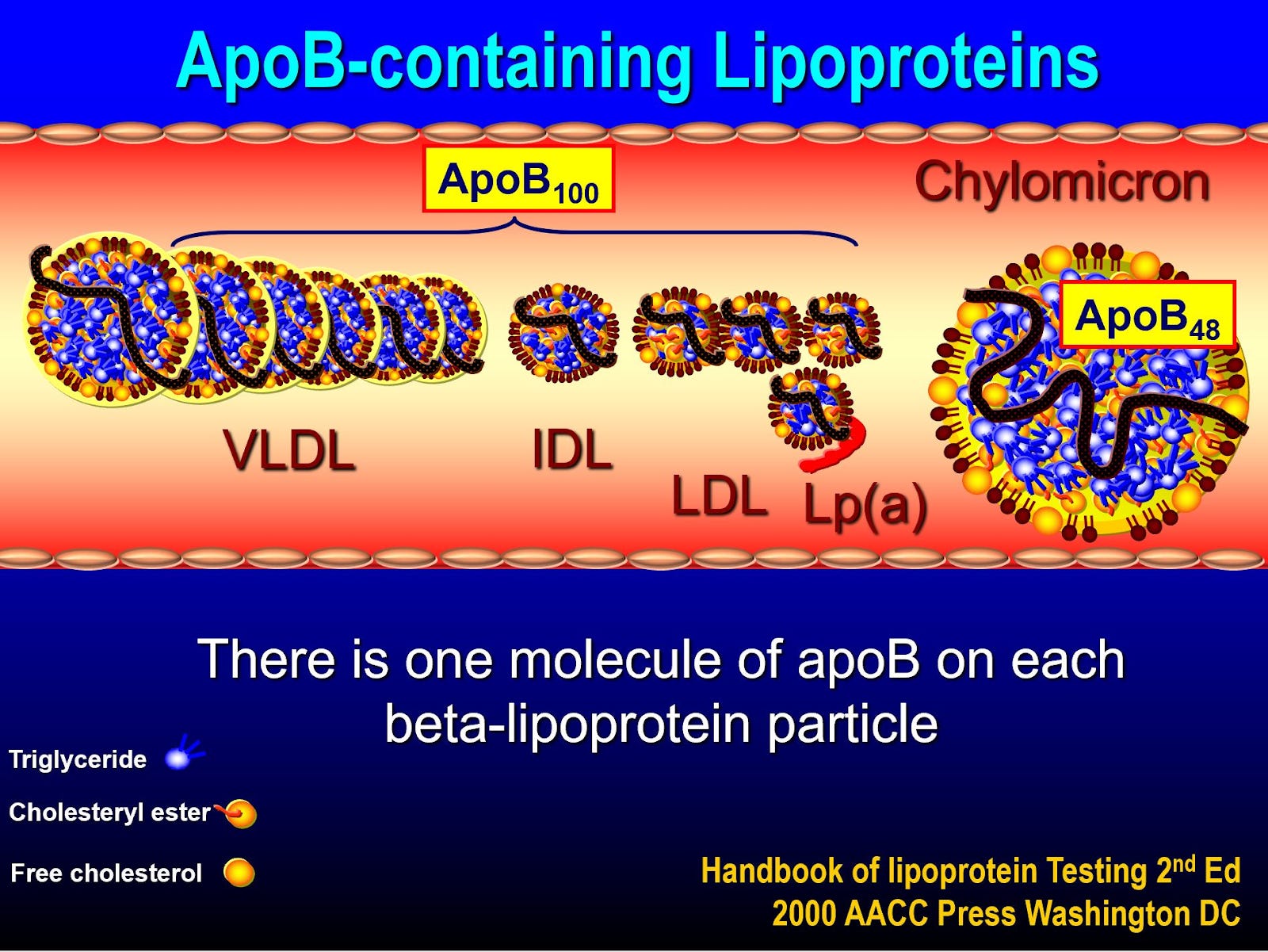
Apolipoprotein B (apoB) measures the concentration of all particles that carry the apoB lipoprotein which includes:
Low-density lipoprotein (LDL)
Very low-density lipoprotein (VLDL)
Intermediate-density lipoprotein (IDL)
Lp(a)
Many doctors use LDL concentration as a predictor of your Atherosclerotic Cardiovascular Disease (ASCVD) risk.
The higher your number, the more at risk you are.
However, apoB is emerging as a better predictor of ASCVD risk because it captures LDL exposure in addition to other particles that drive risk (VLDL, IDL, Lp(a)).
ASCVD Risk Factors
Atherosclerotic Cardiovascular Disease (ASCVD): a group of diseases caused by plaque buildup in artery walls resulting in outcomes such as heart attack or stroke.
There are three causes of ASCVD that we can modify:
Smoking
Hypertension (high blood pressure)
Elevated apoB (too many lipoproteins that have apoB on them: LDL, IDL, VLDL, Lp(a))
Other than not smoking, maintaining a healthy blood pressure and low apoB gives us the best shot at not dying from ASCVD.
Blood pressure
Aim for a blood pressure of 120/80 or below.
Lifestyle factors such as body weight, exercise, and sleep play a big role in maintaining healthy blood pressure.
But if lifestyle changes aren’t working, medications are available to lower your blood pressure. Speak with your doctor.
If your blood pressure is higher than 120/80, you’re exposing yourself to unnecessary risk of disease and death that could be eliminated.
Related reading: Mitigating Disease via Blood Pressure
apoB
ASCVD is caused by circulating, cholesterol-carrying, apoB-containing lipoprotein particles.
The lower your apoB, the lower your risk.
If your LDL-C and apoB are going up, so is your risk of dying from ASCVD.
What apoB should I target?
Depends on who you ask.
Some are more aggressive than others but the consistent recommendation is to lower apoB to 50 mg/dL or below.
For most people, this will not be possible without a combination of nutritional and pharmacological (drug) intervention.
More on that shortly.
Dr. Peter Attia
In episode #599 of The Tim Ferriss Show, Attia states that to eliminate death from ASCVD, you should get your apoB as low as possible as early as possible and that if your LDL-C is below 30 mg/dL and your apoB is below 40 mg/dL for a long time, your odds of suffering ASCVD are incredibly low.
Attia recommends an apoB of 20 to 30 mg/dL (or 30 to 40 mg/dL according to this clip) with 60 mg/dL being the absolute cap.
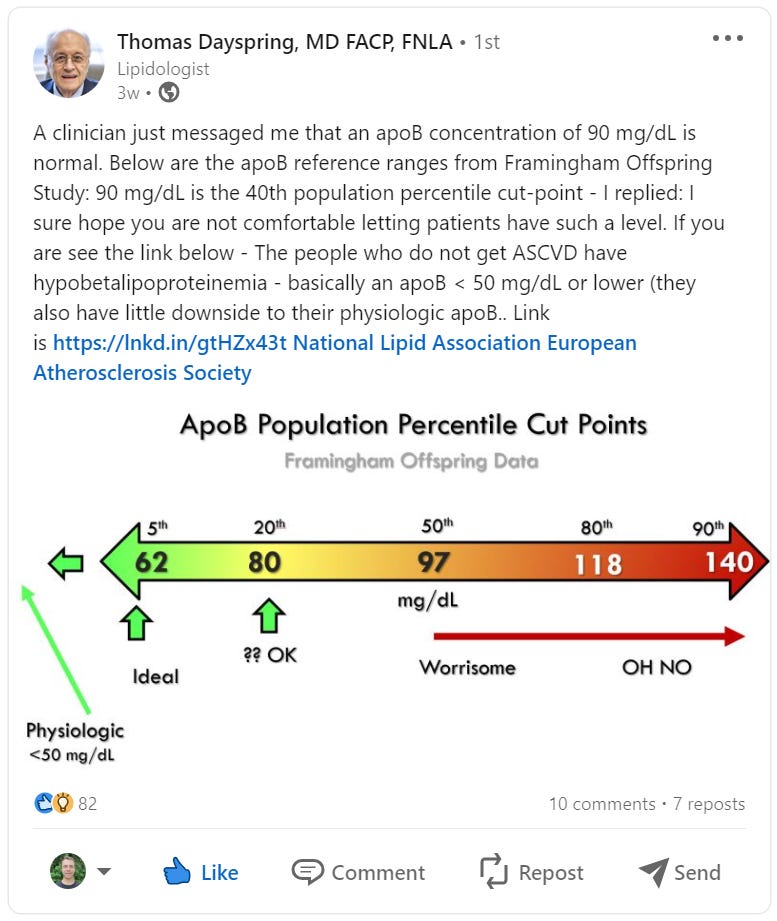
Dr. Thomas Dayspring
Dayspring is the foremost world-leading expert on lipid health.
Based on the post below, Dayspring suggests a sub 50 mg/dL apoB.
“The people who do not get ASCVD have an apoB < 50 mg/dL or lower.” — Dr. Dayspring
Strategies to lower apoB
There are two primary strategies to drive down apoB: nutrition and drugs.
Drugs are the most potent way to impact your lipid health but nutrition still plays a significant role.
Exercise
Although exercise has no meaningful impact on lowering ASCVD risk through influencing lipoproteins, it substantially lowers your risk of ASCVD and other horseman diseases in different ways (i.e., lowering blood pressure and heart rate, improving metabolic health, etc.).
Exercise is critical.
Get in your long-duration zone two, high-intensity zone five, and strength training every week.
Nutrition
To lower your apoB via nutrition, there are two primary levers you can pull:
Dramatically reduce carbohydrate intake.
Dramatically reduce saturated fat intake.
On a very low carbohydrate and very low saturated fat diet, your apoB would drop.
However, this would be a very restrictive diet and for most people only intervening via nutrition would not lower your apoB enough to make ASCVD risk irrelevant.
Low Carbohydrates
Triglycerides: a type of fat (lipid) found in your blood.
By dramatically reducing carb intake, your triglycerides will drop. All else equal, the lower your triglycerides the lower your apoB burden.
Low Saturated Fat
Cutting saturated fat from your diet does two things:
Reduces cholesterol synthesis.
Cholesterol synthesis: the production of cholesterol within our bodies, most of which occurs in the liver.
The liver will pull more LDL out of circulation. When saturated fat is lowered, the liver will upregulate LDL receptors so it can pull in more LDL which means less LDL is in circulation.
Conversely, in a high saturated fat diet, cholesterol synthesis increases and LDL receptors are downregulated which results in more apoB-bearing LDL particles circulating through your arteries.
Naive Nutrition
When I stumble across someone preaching how “healthy” butter, cream, tallow, and other high-saturated fat products, I have a strong urge to take a baseball bat to their femurs.
In boldly claiming how great these products are without caveat, they dismiss science and ignorantly violate every rule of nutrition.
Everyone is different and you don’t know something is healthy unless you track key biomarkers in your response to eating it.
While some people can eat extreme levels of saturated fat — as one would on the ketogenic diet — with near impunity, others cannot so much as look at a piece of bacon without sending their apoB skyrocketing.
Do not eat a high saturated fat diet without measuring your apoB and LDL response.
And ignore anyone who fails to consider the nuance and complexity of these topics while dismissing science that refutes or complicates their overly simplistic claims.
High Fiber
High fiber diets have been shown to help manage lipid burden.
Most fiber recommendations undershoot the optimal amount. Aim for the below:
Males: 45 to 50g of fiber per day.
Females: 35 to 40g of fiber per day.
Cholesterol Awareness
While most of the cholesterol you consume is simply excreted without making it into your bloodstream, it’s another lever you can play with to see how modifying your intake impacts your apoB and LDL.
The Mediterranean Diet
The Mediterranean diet (more monounsaturated fats, fewer refined carbs, whole grains high in fiber, vegetables, beans, and fatty fish) may be worth experimenting with to improve your lipid health.
Manage Calories
Consuming excess calories causes a plethora of health issues.
To mitigate your risk of ASCVD and other diseases, strive to consistently eat at or below your maintenance calorie intake, maintain a healthy body weight, and minimize your consumption of junk food.
The Bottom Line
Meaure. Measure. Measure.
How your diet makes you feel is important but it’s just the tip of the iceberg.
To gain a full picture how of your nutrition is impacting your health, you must measure and track important biomarkers. In the case of ASCVD, those biomarkers are apoB, LDL, and Lp(a).
You could feel and look great but have elevated apoB or Lp(a) causing you to die suddenly and prematurely from a heart attack or stroke.
To determine how your diet is influencing your ASCVD risk, ask your doctor for a requisition for a lipid panel. Alternatively, you can pay a private company such as Inside Tracker for these tests.
Lipid-Lowering Medications
While diet is important, drugs have a much larger impact on lowering apoB.
Here’s an overview of lipid-lowering medications based on Outlive by Peter Attia.
Use this information to discuss potential solutions with your doctor.
Statins
Statins are the starting place for most people with elevated lipids.
There are different types of statins, but most start on rosuvastatin (CRESTOR) and pivot if negative side effects arise. An alternative statin is pitavastatin (LIVALO).
Although rosuvastatin is dosed up to 40mg, you get around 85% of its maximum apoB reduction at a 5mg dose. There’s no reason to go any higher than a 10mg dose because you’re just buying negative side effects without much, if any, additional benefit.
Statin side effects:
Muscle aches/soreness
Elevations of transaminases (liver function tests)
Insulin resistance
Muscle aches will be obvious and the other two can be monitored with tests.
Speak with your doctor to create a strategy to track your liver function and metabolic health (insulin resistance) if you start statins.
In a risk-benefit-cost analysis, statins are a great tool for many people.
They’re extremely cheap and effective, any negative side effects can be reversed by stopping them, and the cost of inaction (dying from a heart attack or stroke) is much higher than the cost of action (if monitored, you can stop taking statins to prevent the continuation of negative side effects).
Bempedoic acid
For those who cannot tolerate statins, another option is bempedoic acid (NEXLETOL).
The main drawback of this drug is the cost.
Ezetimibe
Ezetimibe (Zetia) blocks the absorption of cholesterol in the GI tract.
It works well when taken in combination with a statin because statins, which block cholesterol synthesis (the production of cholesterol in our bodies), tend to increase cholesterol reabsorption in the gut which is exactly what ezetimibe prevents.
PCSK9 inhibitors
PCSK9 inhibitors are an emerging drug that improves the liver’s ability to clear apoB.
Taking both a statin and PCSK9 inhibitor is the most deadly tool we have against apoB.
Additionally, while statins cannot reduce Lp(a), another deadly particle that wildly increases ASCVD risk, PCSK9 inhibitors can reduce it by around 30%.
Fibrates
Fibrates can lower triglycerides if you are not able to do so via nutritional intervention.
Ethyl eicosapentaenoic acid (EPA)
Ethyl eicosapentaenoic acid (VASCEPA), the EPA component of fish oil supplements, contains four grams of EPA and is cleared by the FDA to reduce LDL in patients with elevated triglycerides.
Taking a high-quality fish oil supplement which contains both EPA and DHA, such as those from Nordic Naturals or Carlson Labs, may also improve heart health and reduce ASCVD risk.
Attia’s Personal Protocol
Peter Attia takes three drugs to lower his apoB and mitigate his risk for ASCVD:
PCSK9 Inhibitor: Repatha. There are two FDA-approved PCSK9 inhibitors: alirocumab (PRALUENT) and evolocumab (Repatha).
NEXLIZET: One pill that is a combination of bempedoic acid and ezetimibe.
Statin: He didn’t mention it in the clip but I believe he takes rosuvastatin.
He takes a plethora of supplements for many reasons including a standard EPA and DHA containing fish oil such as those mentioned above.
Next Steps
If this is all new to you, begin by asking your doctor for a bloodwork requisition for a full lipid panel including apoB and Lp(a).
Ask them to include a liver function test in the requisition (I believe most doctors use Alanine Aminotransferase (ALT)) so that if you end up taking a statin you have a starting baseline to measure liver function.
The medical system is organized to fight disease once it’s taken hold, not proactively prevent it (read more on the lethal flaws of our medical system here).
So most doctors will look at you like you have a second head when you try to drive your apoB below 50 mg/dL.
Be patient and persistent. Ask questions. Do more research by listening to one of Peter Attia’s many podcasts on this topic or scrolling through Thomas Dayspring’s X or LinkedIn.
With consistent and proactive determination, you will implement the nutritional, exercise, and sleep practices in your own life and work with the medical system to ensure you have the right drug strategy to drastically reduce or eliminate your risk for the number one cause of death in the world.
An ask: If you enjoyed this post, please hit the heart ❤️ and share it with a friend. It helps me understand which topics you value and supports the growth of this publication.
Much love,
Jack
Thanks for this post. Funnily enough, after reading your Attia book summary, I'd made a note of this to ask my doc for at a physical earlier this week.
They unfortunately stuck me with an older doc I'd never met, and he was 100% not interested in hearing about apoB, or anything else outside of flowchart medicine from decades ago. I gently persisted, asking if due to family cardiac history I could get this added to my bloodwork. He got visibly angry, jaw clenched, and said, "I am not interested in alternative medicine." I said, "Or modern research, apparently," which was when he stormed out of the physical in a huff. So, all of that to say, not all doc's are on board with this. I hope that changes.
I did just find that Inside Tracker has added this to their screening, though their plans are very expensive (~$700 for the most basic testing plan). Still, could be money well spent if one can't find a doctor who will order this test.